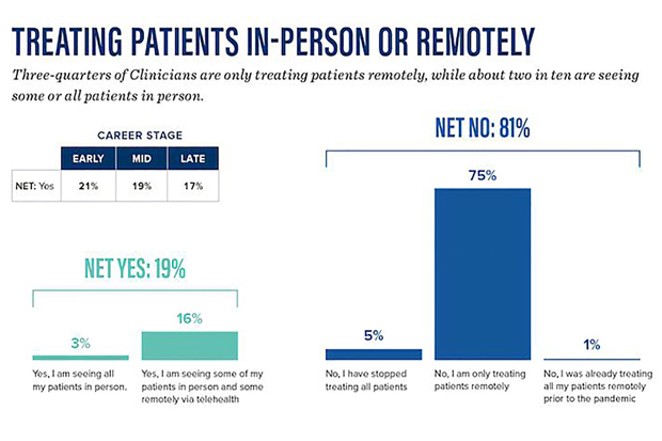
With the declaration of a Public Health Emergency in the U.S. in 2020, mental health therapists, psychologists and other clinicians were able to make a quick pivot to teletherapy—therapy administered by either telephone or video conferencing. According to a survey by the American Psychological Association published in June, 75% of clinicians reported treating patients remotely. Only 1% of clinicians reported doing so prior to the pandemic.
Now, with COVID-19 vaccines being distributed and hope for a return to some semblance of normalcy on the horizon for 2021, will patients and clinicians return to the in-person model?

For some patients, that might come down to whether their insurance company—or Medicare—decides to allow teletherapy following the Public Health Emergency.
In light of this Mental Health Issue, we checked in with a local therapist about the pros and cons. Our email conversation has been condensed for space.
Alicia Viani is a mental health therapist and a Licensed Clinical Social Worker who works in private practice after many years as a therapist in community mental health clinics. She sees individual youth and adults, and couples and families.
Source Weekly: Did you do any teletherapy before the pandemic?
Alicia Viani: I had never before had any experience with teletherapy. On occasion a client would need to have a phone session, but this required either a special insurance pre-authorization or for the client to self-pay and not utilize insurance, which can be burdensome because therapy is expensive.
SW: What did a session look like before the pandemic?
AV: Typical pre-pandemic sessions were 55-minute in-person meetings in my office. In session, my clients and I used our strong relationships to process emotion and somatic experience related to trauma, which involved a warm emotional closeness, eye contact, doing EMDR, somatic processing and moving around the office, sitting on the floor together, occasional art therapy, and we’d practice mindfulness and regulation together.
SW: Describe what it looked like, transitioning to teletherapy.
AV: My practice transitioned exclusively to teletherapy in the spring of 2020. Despite us being “essential workers,” we were advised by the state and our licensing boards to provide phone or online sessions whenever possible. This was a good thing, because it helped with curving the pandemic. It was and is also very challenging, because we have a national and international mental health crisis on our hands and it’s apparent in how many people I know and have worked with for a long time are struggling more acutely. The uncertainty, anxiety, loneliness, and grief with this pandemic are challenging enough on their own, but they also exacerbate other issues. Disordered eating and substance abuse issues have skyrocketed.
As many, not all, clients’ struggles increased, I noticed I felt my ability to connect with and support them at the level I wanted decreased. I’m grateful our relationships persisted at all thanks to mental health lobbyists and insurance companies who immediately ensured coverage of telehealth services. Clients regularly verbalize their appreciation of that: even though everything else has changed, our relationship and the line of support could remain intact.
But it feels different. It’s impossible to make eye contact via Zoom. When there’s a glitch in the internet connection we end up talking over each other or miss words or expressions, and even though our logical executive functioning brain knows it’s just an internet glitch due to a pandemic because everyone in our neighborhoods (is) online, our lower social/emotional processing brains can interpret that as a threat in a relationship or the therapist being mis-attuned and not fully present, which are critical qualities for the healing relationship.
And most importantly, the pandemic launched many people into further crises where basic needs were threatened or unmet. I had clients become homeless during the pandemic and due to job loss, poverty increased for many. Inability to access social services like unemployment or disability services in schools or in the community put enormous strain on clients. People with vulnerable gender or racial identities feel the pandemic more acutely because institutional racism on top of limited jobs, access to services and people on the street with short tempers equals more trauma. While people around the country talked about embracing “home time” and “getting closer with families,” that’s extraordinarily difficult for people whose families aren’t safe. School and work are lifelines for many and where they could access safe relationships and have a break from homes that aren’t nurturing.
SW: I’ve read some accounts of clients who benefited from teletherapy in that the therapist was able to address their challenges directly in the space where the person was facing them. Have you had experiences like that?
AV: Some clients identify this time as helping make therapy way more accessible to them practically and emotionally. Closeness and intimacy with another person can bring up painful emotions that are dysregulating for a lot of people. The screens and distance help them have less relational stimulation so they can access their feelings. I have clients with new babies who can access therapy more practically while they’re at home. There have actually been many times where clients have identified teletherapy as working well for them and they are flourishing. The majority say they miss in-person connection and the type of work we can do.
SW: Describe any privacy issues you might have encountered due to people doing therapy in their homes or other more public places, rather than at your office.
AV: Therapy is completely dependent on having confidentiality so clients can say whatever they need to without worrying who might hear and what might come of that. Usually I'm in control of confidentiality by having sessions in my office with sound machines running. Since clients are now in control of their own privacy, this is challenging for some. I've done many many sessions with people in their cars. Someone was huddled in a closet. Others were in laundry rooms or other random places in their homes. Many go for walks. With the weather changing, this is harder. Unfortunately, a couple of people who don't have safety in their homes felt too vulnerable and therefore stopped therapy or missed sessions due to not feeling safe speaking freely. I worry about these folks.
SW: What’s your read on your clients’ desire to continue teletherapy?
AV: The majority want to return to in-person because therapy is based on relationship and the emotional, somatic, and physical nature of relationship such as facial mirroring and eye contact are easier. I also know my own strengths and how I can best benefit my clients, and I operate best in-person, so I will be making that transition whenever it's safe to do so. In the meantime however, I'm grateful to have a job, to keep continuity via a stable, caring relationship with folks who need it, and to provide support.
SW: It’s clear that 2020 has wrought a mental health crisis for many, many people. What is your hope for addressing this crisis in 2021?
AV: We are certainly in a mental health crisis. My hope is that since mental health vulnerability is on our minds and more part of the national conversation, this will decrease the stigma and shame in receiving services. I hope we all have increased compassion for how isolation, anxiety, and loss impact day-to-day functioning and to embrace the notion that everyone needs some help from time to time and this isn’t a shameful thing. I also hope that access continues to increase for people both in coverage as well as unique ways to receive services such as expanded telehealth. And, I hope that we talk more about the invisible issues we love to avoid that are worsening due to the pandemic. Where is the talk on the national stage about undocumented people who not only lost jobs but are afraid to access services including health care? Or increased homelessness and poverty in a culture who still think these are issues of laziness?
Telehealth has expanded mental health services for many and some people in isolation with vulnerable identities like being trans in rural communities can access help better, but we still have a long way to go in acknowledging mental health, taking accountability as a society for how we increase certain people’s pain more than others due to our dominant white privilege culture, and ensuring everyone has equal and safe access to care since our system of mental health still benefits privileged groups over more vulnerable ones.
Now, with COVID-19 vaccines being distributed and hope for a return to some semblance of normalcy on the horizon for 2021, will patients and clinicians return to the in-person model?

Adobe Stock
Remote therapy may not be ideal, but it is helping some weather the pandemic.
For some patients, that might come down to whether their insurance company—or Medicare—decides to allow teletherapy following the Public Health Emergency.
In light of this Mental Health Issue, we checked in with a local therapist about the pros and cons. Our email conversation has been condensed for space.
Alicia Viani is a mental health therapist and a Licensed Clinical Social Worker who works in private practice after many years as a therapist in community mental health clinics. She sees individual youth and adults, and couples and families.
Source Weekly: Did you do any teletherapy before the pandemic?
Alicia Viani: I had never before had any experience with teletherapy. On occasion a client would need to have a phone session, but this required either a special insurance pre-authorization or for the client to self-pay and not utilize insurance, which can be burdensome because therapy is expensive.
SW: What did a session look like before the pandemic?
AV: Typical pre-pandemic sessions were 55-minute in-person meetings in my office. In session, my clients and I used our strong relationships to process emotion and somatic experience related to trauma, which involved a warm emotional closeness, eye contact, doing EMDR, somatic processing and moving around the office, sitting on the floor together, occasional art therapy, and we’d practice mindfulness and regulation together.
SW: Describe what it looked like, transitioning to teletherapy.
AV: My practice transitioned exclusively to teletherapy in the spring of 2020. Despite us being “essential workers,” we were advised by the state and our licensing boards to provide phone or online sessions whenever possible. This was a good thing, because it helped with curving the pandemic. It was and is also very challenging, because we have a national and international mental health crisis on our hands and it’s apparent in how many people I know and have worked with for a long time are struggling more acutely. The uncertainty, anxiety, loneliness, and grief with this pandemic are challenging enough on their own, but they also exacerbate other issues. Disordered eating and substance abuse issues have skyrocketed.
As many, not all, clients’ struggles increased, I noticed I felt my ability to connect with and support them at the level I wanted decreased. I’m grateful our relationships persisted at all thanks to mental health lobbyists and insurance companies who immediately ensured coverage of telehealth services. Clients regularly verbalize their appreciation of that: even though everything else has changed, our relationship and the line of support could remain intact.
But it feels different. It’s impossible to make eye contact via Zoom. When there’s a glitch in the internet connection we end up talking over each other or miss words or expressions, and even though our logical executive functioning brain knows it’s just an internet glitch due to a pandemic because everyone in our neighborhoods (is) online, our lower social/emotional processing brains can interpret that as a threat in a relationship or the therapist being mis-attuned and not fully present, which are critical qualities for the healing relationship.
And most importantly, the pandemic launched many people into further crises where basic needs were threatened or unmet. I had clients become homeless during the pandemic and due to job loss, poverty increased for many. Inability to access social services like unemployment or disability services in schools or in the community put enormous strain on clients. People with vulnerable gender or racial identities feel the pandemic more acutely because institutional racism on top of limited jobs, access to services and people on the street with short tempers equals more trauma. While people around the country talked about embracing “home time” and “getting closer with families,” that’s extraordinarily difficult for people whose families aren’t safe. School and work are lifelines for many and where they could access safe relationships and have a break from homes that aren’t nurturing.
While people around the country talked about embracing "home time" and "getting closer with families," that's extraordinarily difficult for people whose families aren't safe. School and work are lifelines for many and where they could access safe relationships and have a break from homes that aren't nurturing. - Alicia Viani
tweet this
SW: I’ve read some accounts of clients who benefited from teletherapy in that the therapist was able to address their challenges directly in the space where the person was facing them. Have you had experiences like that?
AV: Some clients identify this time as helping make therapy way more accessible to them practically and emotionally. Closeness and intimacy with another person can bring up painful emotions that are dysregulating for a lot of people. The screens and distance help them have less relational stimulation so they can access their feelings. I have clients with new babies who can access therapy more practically while they’re at home. There have actually been many times where clients have identified teletherapy as working well for them and they are flourishing. The majority say they miss in-person connection and the type of work we can do.
SW: Describe any privacy issues you might have encountered due to people doing therapy in their homes or other more public places, rather than at your office.
AV: Therapy is completely dependent on having confidentiality so clients can say whatever they need to without worrying who might hear and what might come of that. Usually I'm in control of confidentiality by having sessions in my office with sound machines running. Since clients are now in control of their own privacy, this is challenging for some. I've done many many sessions with people in their cars. Someone was huddled in a closet. Others were in laundry rooms or other random places in their homes. Many go for walks. With the weather changing, this is harder. Unfortunately, a couple of people who don't have safety in their homes felt too vulnerable and therefore stopped therapy or missed sessions due to not feeling safe speaking freely. I worry about these folks.
SW: What’s your read on your clients’ desire to continue teletherapy?
AV: The majority want to return to in-person because therapy is based on relationship and the emotional, somatic, and physical nature of relationship such as facial mirroring and eye contact are easier. I also know my own strengths and how I can best benefit my clients, and I operate best in-person, so I will be making that transition whenever it's safe to do so. In the meantime however, I'm grateful to have a job, to keep continuity via a stable, caring relationship with folks who need it, and to provide support.

American Psychological Association
As this chart shows, most therapists have made the adjustment to remote teletherapy.
SW: It’s clear that 2020 has wrought a mental health crisis for many, many people. What is your hope for addressing this crisis in 2021?
AV: We are certainly in a mental health crisis. My hope is that since mental health vulnerability is on our minds and more part of the national conversation, this will decrease the stigma and shame in receiving services. I hope we all have increased compassion for how isolation, anxiety, and loss impact day-to-day functioning and to embrace the notion that everyone needs some help from time to time and this isn’t a shameful thing. I also hope that access continues to increase for people both in coverage as well as unique ways to receive services such as expanded telehealth. And, I hope that we talk more about the invisible issues we love to avoid that are worsening due to the pandemic. Where is the talk on the national stage about undocumented people who not only lost jobs but are afraid to access services including health care? Or increased homelessness and poverty in a culture who still think these are issues of laziness?
Telehealth has expanded mental health services for many and some people in isolation with vulnerable identities like being trans in rural communities can access help better, but we still have a long way to go in acknowledging mental health, taking accountability as a society for how we increase certain people’s pain more than others due to our dominant white privilege culture, and ensuring everyone has equal and safe access to care since our system of mental health still benefits privileged groups over more vulnerable ones.